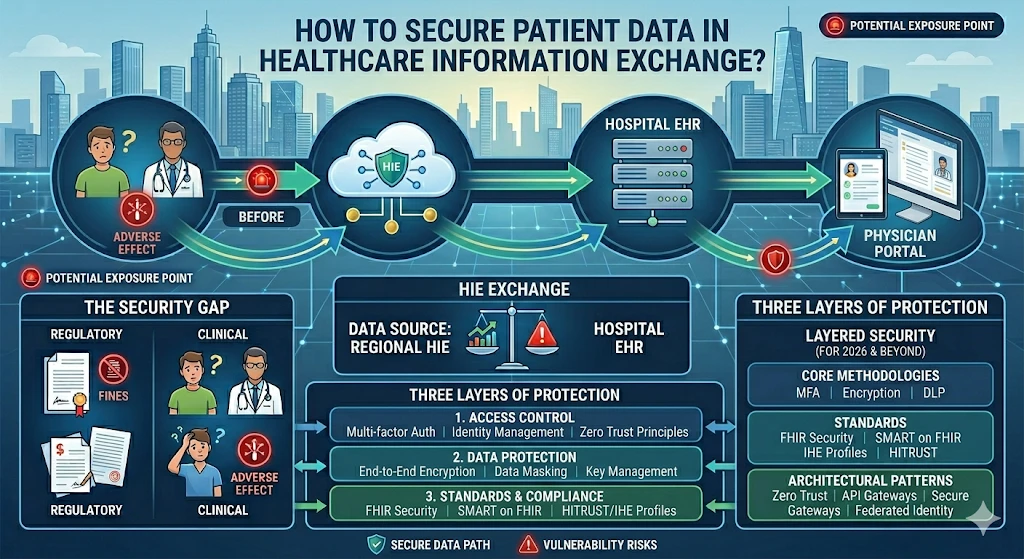
How to Secure Patient Data in Healthcare Information Exchange?


A patient's lab result travels from a reference lab to a primary care physician, gets routed through a regional HIE, lands in a hospital EHR, and surfaces in a specialist's portal, all within hours. Every handoff in that chain is a potential exposure point. And when something goes wrong, the consequences are not just regulatory. They're clinical.
Healthcare data breaches have become the most costly of any industry, averaging over $10 million per incident in recent years. Yet the volume of data moving through health information exchanges keeps climbing. Interoperability mandates require it. Value-based care models depend on it. The challenge is not whether to share patient data — it's how to do it without creating unacceptable risk.
Securing patient data in healthcare information exchange requires more than deploying encryption or ticking a HIPAA compliance box. It demands a layered, architecture-level approach that accounts for the full complexity of modern clinical data flows — across organizations, systems, and regulatory jurisdictions.
This article walks through the core security methodologies, standards, and architectural patterns that healthcare organizations and their technology partners need to implement in 2026 and beyond.
Why Health Information Exchange Security Is More Complex Than It Looks
Most healthcare organizations understand the basics: encrypt data in transit, enforce access controls, maintain audit logs. The problem is that HIEs don't operate like internal systems. They're inherently multi-organizational, multi-vendor environments where data moves across trust boundaries constantly.
A single patient record might be accessed by a primary care provider, a cardiologist, a pharmacy benefits manager, a care coordinator, and a population health analytics platform, each running different software, with different authentication systems, under different organizational security policies.
Understanding these dynamics is essential before you can solve them. Alongside authentication gaps and unencrypted data flows, the broader structural and organizational health information exchange challenges — from governance fragmentation to inconsistent data standards — make securing patient data significantly harder than most organizations anticipate.
Three specific dynamics make health information exchange security particularly difficult:
- Federated identity: There's no universal identity provider across HIE participants. A clinician authenticated in System A is a stranger to System B, and mapping identities across organizations without creating new attack surfaces is genuinely hard.
- Data format heterogeneity: HL7 v2 messages, C-CDA documents, FHIR resources, and proprietary formats often coexist in the same exchange. Each transformation step is a point where validation can fail or data can be misrouted.
- Asymmetric security maturity: A large academic medical center and a two-physician rural practice may both participate in the same HIE. Their security capabilities are not comparable — and the weakest link defines the exposure.
Core Methodologies for Securing Patient Data in Healthcare Information Exchange
1. End-to-End Encryption — In Transit and At Rest
Encryption is the baseline. But "encrypted" is not a binary state in HIE environments — it's a spectrum that requires deliberate architecture decisions at every layer.
For data in transit, TLS 1.2 is the minimum; TLS 1.3 should be the standard for any new implementation. All API connections — including FHIR RESTful endpoints, SOAP-based legacy interfaces, and Direct messaging channels — must enforce TLS without exception. Certificate pinning should be applied where the endpoint set is predictable.
For data at rest, AES-256 encryption of database fields containing PHI is standard practice. But field-level encryption matters too: a database encrypted at the volume level can still expose sensitive fields if an application layer vulnerability allows direct queries. Envelope encryption — where data encryption keys (DEKs) are themselves encrypted by master keys managed in a hardware security module (HSM) — provides an additional layer.
Database-level encryption alone is not sufficient. Backup files, audit logs, and cached query results all represent vectors where unencrypted PHI can escape the primary data store.
2. Zero Trust Architecture for HIE Environments
The traditional perimeter security model — trust everything inside the network, block everything outside — was already struggling before HIEs became mainstream. In a multi-organizational exchange environment, it doesn't apply at all. There is no perimeter.
Zero Trust Architecture (ZTA) operates on a different principle: no user, device, or service is trusted by default, regardless of network location. Every access request is authenticated, authorized, and continuously validated. For HIE environments, this means:
- Identity verification at every API call, not just at session initiation
- Device posture checks before granting access to PHI — unmanaged or non-compliant devices are denied regardless of user credentials
- Microsegmentation of the data environment so that a compromised application cannot pivot laterally to patient record stores
- Continuous monitoring with real-time anomaly detection, not periodic audits
Implementing ZTA in a secure information exchange architecture is not a single-vendor product deployment. It's an organizational posture shift that requires buy-in at the infrastructure, application, and governance levels simultaneously.
3. FHIR Security and SMART on FHIR Authorization
As FHIR R4 becomes the dominant exchange standard under ONC mandates, its security model deserves specific attention. FHIR itself is a data model and API specification — it doesn't prescribe authentication. That's where SMART on FHIR comes in.
SMART on FHIR extends OAuth 2.0 for healthcare contexts, enabling fine-grained, patient-context-aware authorization. Rather than granting a consuming application access to all patient records, SMART scopes define exactly what resources an application can read or write, and for which patients.
Key SMART on FHIR security controls to enforce in any HIE deployment include:
- Mandatory use of PKCE (Proof Key for Code Exchange) for all authorization code flows
- Scope validation on every API request, not just at token issuance
- Short-lived access tokens (15–60 minutes) with refresh token rotation
- Launch context enforcement to bind application access to specific patient encounters
- Audience validation to prevent token replay attacks across services
For backend service integrations — where there's no human user initiating the OAuth flow — the SMART Backend Services specification uses asymmetric key authentication (JWT client assertions) instead of client secrets. This eliminates the shared-secret vulnerability common in machine-to-machine integrations.
4. Attribute-Based Access Control (ABAC)
Role-Based Access Control (RBAC) assigns permissions based on job role: physicians can read records, nurses can update vitals, billing staff can access financial data. It's a reasonable starting point, but it doesn't capture the full complexity of clinical access decisions.
Attribute-Based Access Control evaluates a richer set of conditions before granting access: not just who the user is, but what their relationship to the patient is, what time it is, what device they're using, what purpose they've declared, and what regulatory context applies. An ABAC policy might allow an emergency physician to access a patient's full record during an active encounter, but restrict access to the same record for the same physician 48 hours after discharge.
In HIE environments, ABAC is particularly important for managing:
- Sensitive data categories (behavioral health, HIV status, substance use disorder) that carry additional legal protections under 42 CFR Part 2 and similar regulations
- Break-glass access scenarios where emergency override is permitted but logged with mandatory follow-up review
- Patient consent directives that restrict which organizations or providers can access specific data elements
Key HIE Security Standards and Frameworks
Compliance is not a security strategy — but the major HIE security standards provide a useful framework for prioritization. Here's how the key frameworks map to specific security domains:
Most mature HIE deployments need to satisfy multiple frameworks simultaneously. The practical reality is that HIPAA sets the legal floor, NIST provides the technical blueprint, and FHIR-specific standards handle the modern API layer. A comprehensive hie security standards program addresses all three levels.
Audit Logging and Continuous Monitoring
Immutable Audit Trails
Every access to patient data in an HIE must be logged — who accessed what, when, from where, and for what purpose. That's not just good practice; it's a regulatory requirement under HIPAA and a core component of any defensible security posture.
The HL7 FHIR AuditEvent resource provides a standardized structure for capturing these events in FHIR-native environments. For legacy systems, IHE's ATNA (Audit Trail and Node Authentication) profile defines how audit messages should be formatted and transmitted over secure syslog.
Audit logs must be:
- Immutable — write-once, tamper-evident storage prevents retroactive modification
- Complete — capturing failed access attempts, not just successful ones
- Centralized — aggregated across all HIE participant systems into a single SIEM
- Retained — at minimum six years under HIPAA, though longer retention periods are prudent
Anomaly Detection and Behavioral Analytics
Audit logs are retrospective. By the time a compliance team reviews them, a breach may be weeks old. Real-time anomaly detection changes the equation.
Modern SIEM platforms with machine learning capabilities can establish behavioral baselines for individual users and flag deviations: a physician querying 300 records in an hour when their baseline is 15, a service account accessing PHI at 3 a.m., a user authenticating from two geographically impossible locations within 30 minutes. These signals, individually ambiguous, become actionable when correlated.
For HIE environments specifically, anomaly detection should be tuned for common attack patterns: credential stuffing against provider portals, lateral movement from compromised API integrations, and bulk data extraction that might indicate an insider threat or compromised third-party application.
Secure Information Exchange Architecture: Centralized vs. Federated
How patient data is physically and logically organized has direct security implications. Two dominant architectural patterns exist in HIE deployments, each with distinct security trade-offs:
Neither architecture is inherently superior from a security standpoint. A centralized model offers simpler audit and consent management but concentrates risk. A federated model distributes risk but requires every participant to maintain adequate security controls — which brings us back to the asymmetric maturity problem.
Hybrid approaches — where a centralized index or record locator service (MPI) manages patient matching without centralizing PHI — are increasingly common and often represent the best balance for large regional or national HIEs.
yber
Third-Party and Vendor Risk Management
In any HIE, the security of the exchange is bounded by the security of its least-secure participant. That means vendor and third-party risk management is not optional — it's structural.
Every organization connecting to an HIE should require:
- Current HIPAA Business Associate Agreements (BAAs) with all technology vendors handling PHI
- SOC 2 Type II reports reviewed annually, not just collected at onboarding
- Penetration testing results — at minimum annually, ideally after significant system changes
- Documented incident response plans with defined notification timelines
- API security assessments for any application consuming or producing FHIR resources
Third-party application access through SMART on FHIR APIs deserves particular scrutiny. The OAuth consent model allows patients (or organizations) to authorize applications to access their data, but that authorization needs to be time-bounded, scope-limited, and revocable. A dynamic client registration process with ongoing monitoring of application behavior is significantly more secure than static API key management.
How to Prevent Cybersecurity Attacks in Healthcare
Patient Consent Management as a Security Control
Security and consent are often treated as separate concerns — security teams handle encryption and access controls, while compliance teams manage consent forms. In reality, patient consent directives are a form of access control policy, and they need to be enforced at the data layer, not just documented on paper.
FHIR Consent resources provide a machine-readable format for capturing patient consent decisions that can be evaluated programmatically at query time. When a provider requests a patient's behavioral health records, the system can check the applicable Consent resource before releasing data — rather than relying on a human workflow to catch exceptions.
For HIEs operating under 42 CFR Part 2 (substance use disorder) or state-specific mental health privacy laws, automated consent enforcement isn't just a convenience. It's a legal requirement that manual processes routinely fail to satisfy at scale.
Conclusion: Security as Architecture, Not Afterthought
Securing patient data in healthcare information exchange is not a problem you can solve with a single tool, standard, or certification. It requires treating security as a first-class architectural concern — built into the design of data flows, API surfaces, identity systems, and governance structures from the ground up.
The organizations that do this well share a few common traits: they apply Zero Trust principles rather than perimeter thinking, they implement FHIR security controls and SMART on FHIR authorization with the same rigor they apply to clinical workflows, they maintain real-time visibility into data access through centralized audit and anomaly detection, and they manage third-party risk as an ongoing program rather than a one-time vendor questionnaire.
Health information exchange security will only grow more complex as interoperability mandates expand, as more applications connect through FHIR APIs, and as the volume of patient data in motion increases. The organizations that invest in secure information exchange architecture now will be far better positioned — technically and legally — than those who treat security as a compliance exercise.
The stakes aren't abstract. Every patient whose data moves through an exchange is trusting that the organizations involved have taken security seriously. That trust is both a clinical responsibility and a strategic one.